Business Statistics & Analytics Homework Help
Stuck on a question? Need homework help? Ask your question and complete your homework assignment!
- *

- * Select Question Subject
- * Select SubjectAll Subjects
- * Filter answersAll Questions
The following patient measurements are taken from a ventilator with an inline oxygen analyzer located at the endotracheal tube/ventilator connection.
What is the patient's O2 consumption.
VT = 600 ml
Resp Rate = 10
FiO2 = .63
FeO2 = .58
Group of answer choices
280 ml/min.
400 ml/min.
300 ml/min.
350 ml/min.
 0
0
{12+} Expedia Canada Phone Number Customer Service: Step-by-Step Contact Guide
.
1
Exercise 11
George Jack operates a small machine shop. He manufactures one standard product available from other similar businesses, and he also manufactures products to customer order. His accountant prepared the annual income statement shown below:
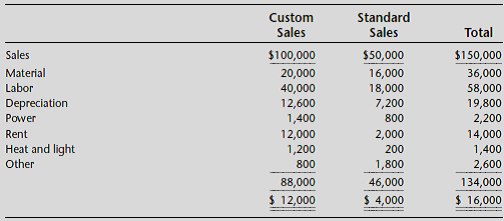
The depreciation charges are for machines. The power charge is apportioned based on estimated power consumed. The rent is for the building space that has been leased for 10 years at $14,000 per year. The rent and heat and light are apportioned to the product lines based on amount of floor space occupied. All other costs are current expenses identified with the product line causing them.
A valued custom parts customer has asked Mr. Jack if he would manufacture 5,000 special units for him. Mr. Jack is working at capacity and would have to give up some other business in order to take this business. He can’t renege on customer orders already agreed to, but he could reduce the output of his standard product by about one-half for one year while producing the specially requested custom part. The customer is willing to pay $16.00 for each part. The material cost will be about $4.50 per unit and the labor will be $8.00 per unit. Mr. Jack will have to spend $4,500 for a special device that will be discarded when the job is done.
Required:
a. Calculate the following costs related to the 5,000-unit custom order.
(1) The differential cost of the order.
(2) The full cost of the order.
(3) The opportunity cost of taking the order.
(4) The sunk costs related to the order.
b. Should Mr. Jack take the order? Explain your answer.
0
The last step in planning a message is adjusting the content to the receiver. true or false?
0
What are the applications of Gene Overexpression Stable Cell Lines?
.
1
Which of the following is/are the correct way(s) to use the following passage without plagiarizing?
“He that readeth good writers and pickes out their flowres for his own nose, is lyke a foole.” - Stephen Gosson Quotes Source: In the School of Abuse--Loyterers
0
Meconium aspiration syndrome
0
How do I delete my Quiz+ account?
0
The “Ancient Kemetic Past” refers to which of the following in the context of African American psychology?
0
When Should an Adolescent Be Treated as an Adult?
Over the past several decades, adolescents have become increasingly involved in what historically have been considered “adult” activities, including violent crime, sexual activity, and substance use. This trend has forced lawmakers to determine, with increasing frequency, whether adolescents who engage in these “adult” activities should be treated as minors (who are deemed incompetent, less blameworthy, and unaccountable) or adults (who are deemed competent and responsible for their own actions).
The ability to evaluate a minor’s level of maturity has thus become very important. For example, does a teenage murderer understand the consequences of his actions? If so, should he be held accountable and punished as an adult? Should a 16-year-old be allowed to seek treatment for a sexually transmitted infection? To make an abortion decision? When is a minor competent enough to be allowed to waive his or her right to counsel during police questioning?
Use these questions to generate 3 guidelines that can help to determine when an adolescent should be treated as an adult. Students will include information about biological, social and cognitive changes that occur in adolescence.
The 3 guidelines should be explained using at least one paragraph each. The guidelines should be rooted in information found in the text and other sources. Your guidelines may be presented as a document or a powerpoint.
0  Ask a new question
Ask a new question 



